
Lecture note
A professional note on Preservé as tissue-preservation thinking: breast surgery is not only a small incision, but a disciplined attempt to respect support structures, vascular and nerve pathways, and patient-specific anatomical limits.
1. Why Preservé should be read as a preservation philosophy
At the Tissue Preservation Preceptorship at Victoriakliniken in Stockholm, Preservé is not best understood as a single technical label. Its educational value is the way it frames breast surgery as a biological support system made of tissue coverage, structural boundaries, neurovascular pathways and patient-specific anatomical limits.
If Preservé is reduced to a small incision or a faster implant placement method, the main lesson is lost. Tissue preservation means minimizing unnecessary tissue disruption, limiting sharp dissection, preserving natural support structures and allowing the patient’s own tissue to contribute to long-term implant stability.
2. Speaker context: Dr. Marie Jaeger and the clinical frame of the course
The speaker context matters in this episode. Dr. Marie Jaeger is presented by Victoriakliniken as a fully qualified plastic, reconstructive and aesthetic surgeon with a particular interest in breast surgery. Her practice includes both primary breast surgery and secondary or revision breast surgery.
That background gives the Preservé discussion a more practical frame. Her public CV records training across Germany and Israel, international fellowships in Italy, the United Kingdom, Switzerland, Sweden and Australia, and a clinical focus that includes breast reconstruction after mastectomy, implant follow-up with ultrasound and Motiva-related educational work.
For RASA, the important lesson is not to copy a named technique mechanically. It is to understand how a centre with follow-up data, revision experience and ultrasound-based assessment places tissue preservation inside a larger discipline: patient selection, pocket accuracy, postoperative monitoring and clear indication limits.

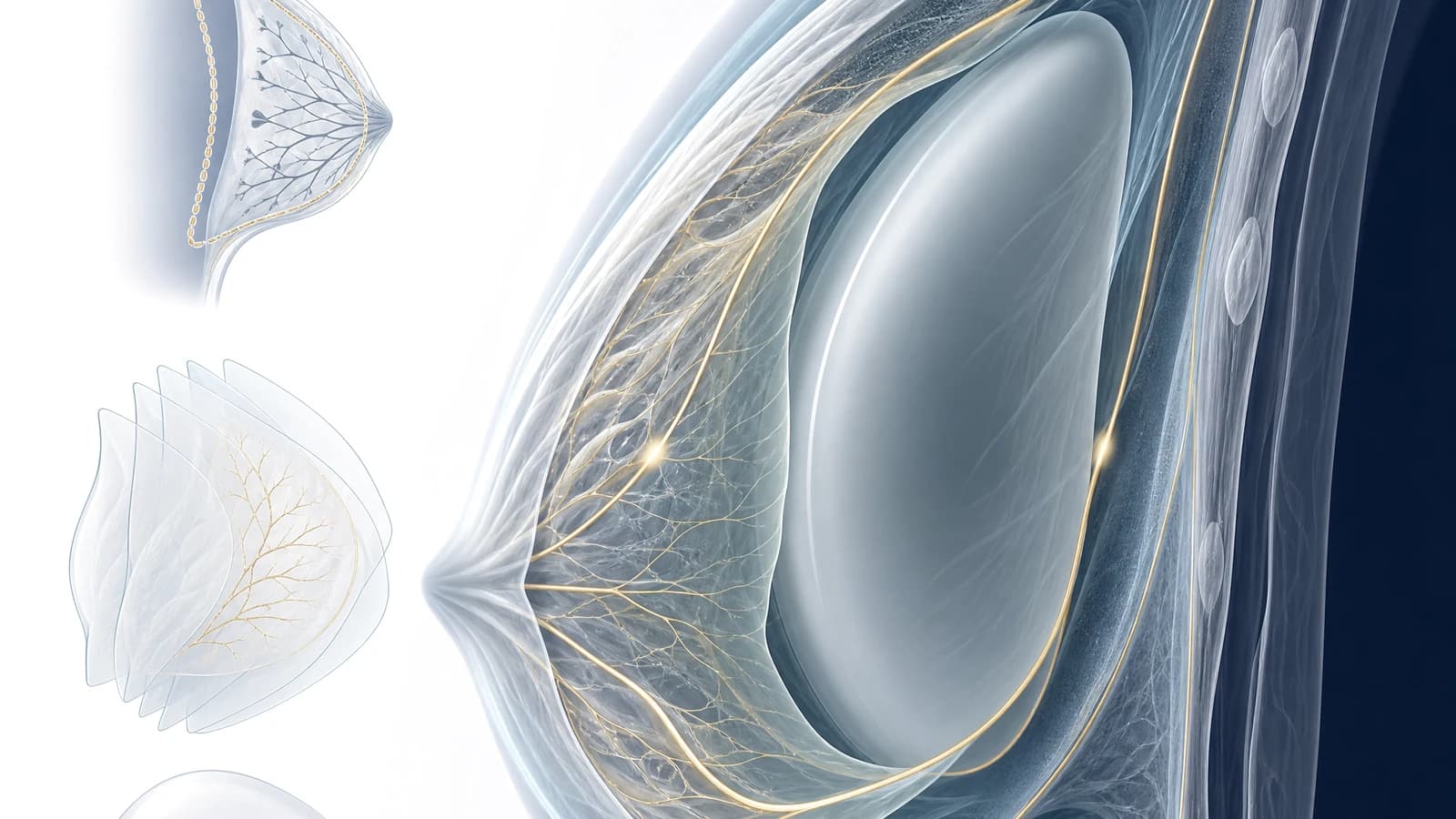
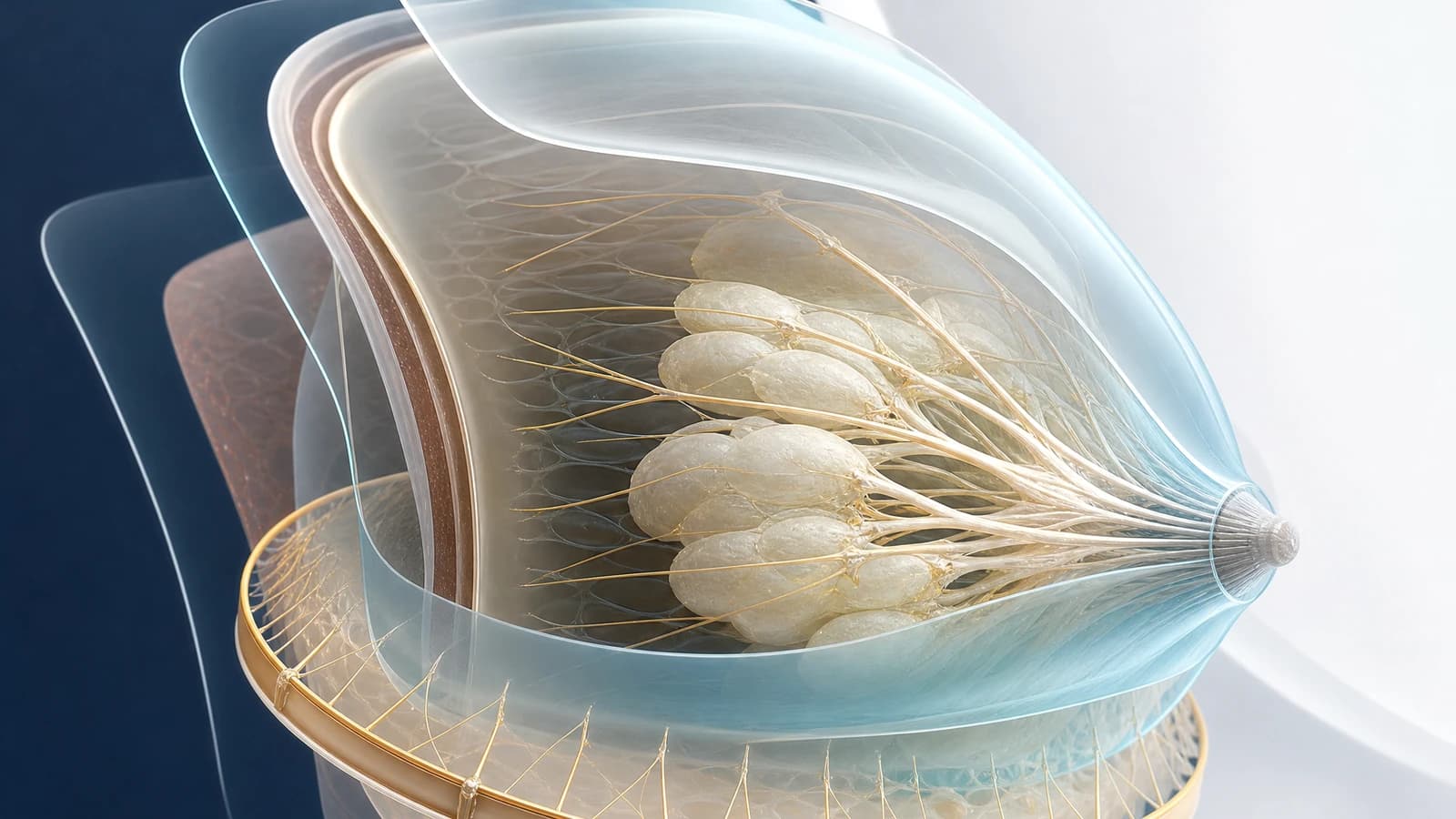
3. Anatomy: laminae, Cooper ligaments and the circum-mammary ligament
The course describes the breast as a three-dimensional system of fat, fascia and fibrous support. The anterior and posterior laminae, Cooper ligaments and circum-mammary ligament help explain why breast shape is not only a matter of implant volume.
In the Preservé concept, the intended pocket is described behind the posterior lamina and above the pectoralis major fascia. The aim is not to create the widest pocket possible, but to stay in a plane that respects the natural support system.
- The laminae help the learner see the breast as a layered support structure.
- The circum-mammary ligament is treated as an anatomical boundary when choosing implant width.
- Pocket creation only makes sense when it matches tissue quality, support and shape goals.
4. Patient selection matters more than volume ambition
A repeated message from the programme is that Preservé is not for every patient. The best candidates are usually those seeking a natural, proportionate change, with good skin and glandular quality, adequate tissue coverage, small-to-moderate volume goals and no need to exceed the natural breast boundary.
Patients with very thin coverage, poor skin quality, major weight loss, scar tissue, prior surgery, large-volume goals or a strong desire for broader implant width may require another strategy. Tissue preservation is therefore a selected indication, not a universal marketing claim.

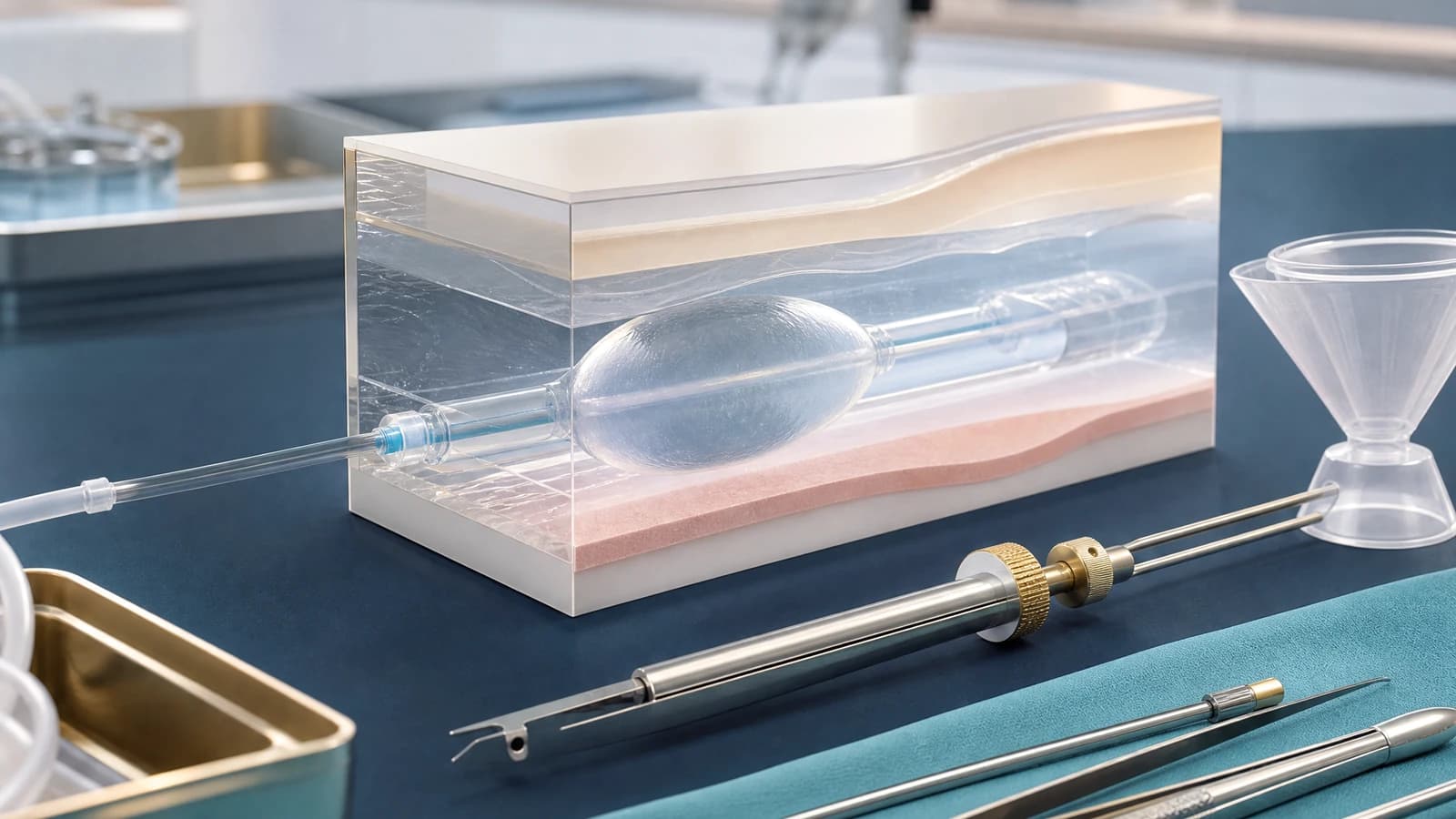
5. Balloon dissection: expanding a pocket instead of cutting one open
Compared with traditional sharp dissection, Preservé uses a channel separator and balloon to expand the pocket with controlled force. The point of the balloon is not simply speed; it is to reduce unnecessary tissue disruption and preserve more of the covering and support structures.
The course describes a “nesting effect”, where the implant sits in a pocket supported by the patient’s own tissue. Still, balloon dissection does not replace anatomical judgement. The surgeon must control the plane, direction, filling volume, symmetry and final implant placement.
- The channel separator must stay in the intended plane above the pectoralis major muscle.
- The balloon must be controlled so it does not drift or overexpand in the wrong direction.
- A good pocket is not the largest pocket; it is the pocket that fits the selected implant and respects anatomical boundaries.
6. Local anesthesia, rapid recovery and communication limits
The programme also highlights awake surgery, walk-in walk-out experience and faster recovery. These points are linked to patient selection, local anesthesia, pain control, standardized workflow and less invasive tissue handling.
The message must remain careful. Awake surgery and same-day discharge do not mean the operation is simple or risk-free. They only make sense when the patient is well selected, pain control is reliable and the indication remains within safe limits.
7. Interpreting clinical data in context
The faculty material discusses thin capsule observations, low inflammatory response, follow-up experience at Victoria Clinic and a dataset involving 660 Motiva implants across Mini, Demi and Full profiles, with a small number of revision decisions within two years.
These details are valuable as course material and centre experience, but they should not be turned into absolute promises for every patient. The larger lesson is how material science, tissue response, patient selection, pocket creation and postoperative care must be read together.
Source material and usage limits
This article is based on Modern Approaches to Tissue Preservation in Breast Surgery at Victoriakliniken, Stockholm, 25-26 May 2026, with Dr. Marie Jaeger identified as the speaker. The programme includes building blocks of breast tissue preservation, technique review, postoperative care, clinical data, silicone model Q&A, markings and TP procedure patients.
It is a RASA Surgical Practice academic interpretation based on the event agenda, RASA educational summary and edited course videos. It does not replace direct medical consultation, implant selection or individualized surgical indication.